
SDG Indicator 3.9.3: Mortality rate attributed to unintentional poisoning
1. Key features and metadata
Definition: This indicator tracks the number of deaths from unintentional poisonings in a year per 100,000 population.
| Sub-indicator | Disaggregated by |
|---|---|
|
SH_STA_POISN Mortality rate attributed to unintentional poisonings, by sex (deaths per 100,000 population) |
Sex (Male/Female)
|
Sources of information: National Statistics Offices, various line ministries and databases covering civil registration with complete coverage and medical certification of cause of death.
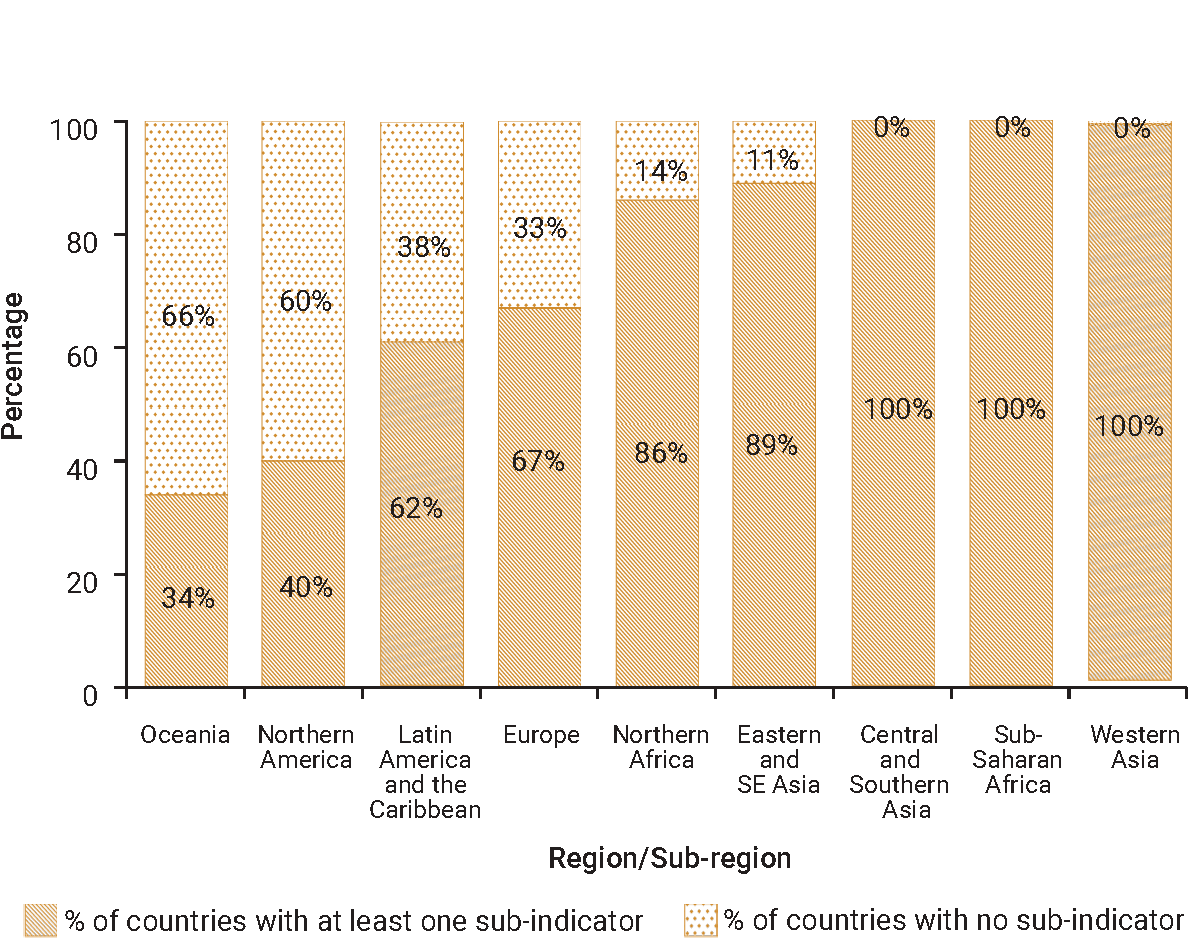
2. Data availability by region, SDG Global Database, as of 02 July 2025
3. Proposed disaggregation, links to policymaking and its impact
| Proposed disaggregation | Link to policymaking | Impact |
|---|---|---|
|
Mortality rate attributed to unintentional poisoning, by age (deaths per 100,000 population) (WHO 2016):
Applies to:
|
This disaggregation provides useful indications for decision-makers on the impacts of unintentional poisoning sources on population health according to their age, the effectiveness of hazardous chemicals pollution management and of the country’s health system (WHO 2017). It also helps identify the most appropriate remedial measures for preventing and reducing related illnesses and risks. For example, the prevention of indoor pollution risks targeted at children and women for substances like lead or pollutants associated with cookstove smoke or second-hand smoke (WHO n.d.d; WHO n.d.e). This disaggregation is in line with the International Health Regulations (IHR)(WHO 2005). |
Exposure to chemical products and natural toxins, pharmaceuticals and pesticides through ingestion, inhalation, skin contact, or the umbilical cord of the unborn child is a major cause of public health concern. Many substances commonly used at home and in the workplace – such as heavy metals, solvents, paints, detergents, kerosene, carbon monoxide, drugs, or pesticides – can lead to unintentional poisonings and increased morbidity. In 2019, 193,000 deaths were estimated to be caused by unintentional poisonings (WHO 2021a). Children as well as pregnant women are more sensitive to poisoning. The production of these substances is increasing and, with it, related health problems. A number of detrimental health impacts of pollution can be significantly reduced through preventive measures and the reduction of exposure to harmful substances. For example, in the case of air pollutants (ambient and indoor) associated with second-hand smoke and the use of leaded gasoline by using modern energy sources and cooking technologies. Other measures should tackle the release of pollution at source from combustion and other energy generation processes, industry or transport through the use of cleaner and efficient resource-use technologies, banning or phasing out harmful substances, new regulatory and control frameworks, and economic incentives. |
|
Mortality rate attributed to unintentional poisoning, by disease (deaths per 100,000 population) (WHO 2021a; WHO 2024):
Applies to:
|
This disaggregation provides useful indications for decision-makers on the impacts of unintentional poisoning on the population health according to the type of illness contracted. It also helps in identifying the most appropriate remedial measures for preventing and reducing those impacts through effective chemical incidents and public health management. For example, promoting the establishment and strengthening of a network of national poisons centers whose role is to advise on the diagnosis and management of poisoning and assure toxicovigilance. This disaggregation is in line with the International Health Regulations (IHR) (WHO 2005). |